Clinical Case Secnario
A 37-year-old male with a long-standing history of chronic smoking (15 pack-years) presented to the emergency department with the acute onset of excruciating, constant, epigastric pain that radiated sharply to his back. This severe pain began approximately 12 hours before presentation and was accompanied by multiple episodes of non-bloody, bilious vomiting and complete loss of appetite (anorexia). He is a chronic smoker (15 pack years) who denies any history of alcohol abuse, recent abdominal trauma, prior surgeries, or known history of gallstones. There has been no history of recent medication intake. Upon admission, he was diagnosed with moderate acute pancreatitis secondary to severe hypertriglyceridemia (serum triglyceride 2902 mg/dL), as supported by initial lab findings and imaging (modified CT scan severity index of 6/10) (Figure 1). He also exhibited signs of systemic inflammatory response syndrome (SIRS), including a fever of 38.5°C on arrival and a respiratory rate of 30 breaths/minute.
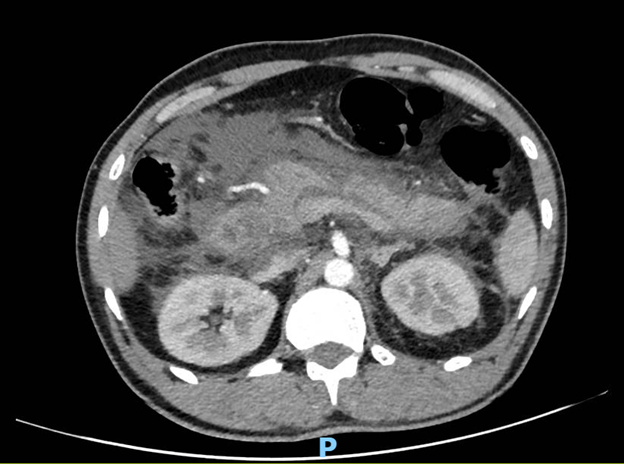
Figure 1: Contrast-enhanced CT abdomen
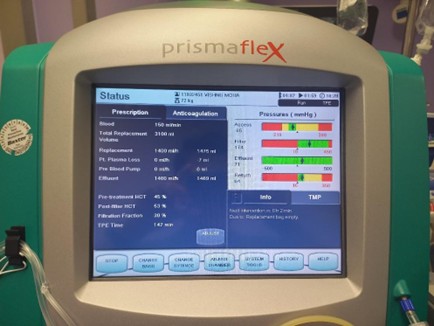
Figure 2: Settings of the extracorporeal therapy

Figure 3: Machine used for extracorporeal therapy
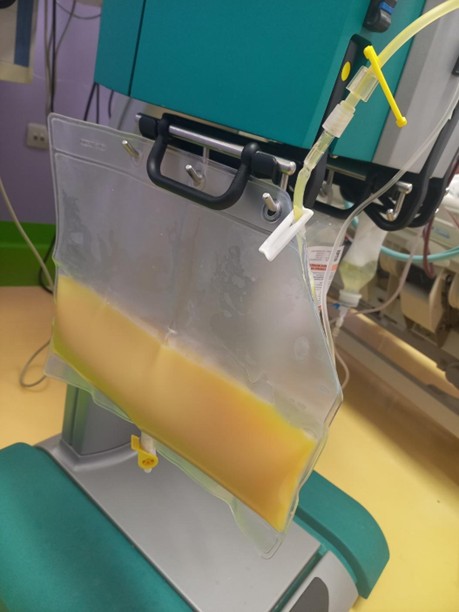
Figure 4: Filtered plasma of the patient, collected as effluent in the bag (yellowish colored as the effluent is lipemic secondary to the high level of triglycerides)
Given the patient's presentation and the ongoing management, which of the following statements regarding the role of the extracorporeal therapy being used (Figures 2, 3, and 4) in hypertriglyceridemia-induced acute pancreatitis is most accurate?