Clinical Case Scenario
A 65-year-old man, 7 months after allogeneic HSCT, develops chronic GVHD treated with steroids and sirolimus. He presents with resistant hypertension, edema, oliguria, proteinuria, and worsening kidney function (Cr 2.95 mg/dL).
Peripheral smear shows no significant schistocytosis. LDH, haptoglobin, and ADAMTS13 are normal.
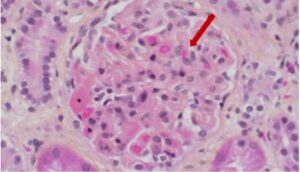
Kidney biopsy reveals endothelial injury, glomerular thrombi, GBM double contours, and arteriolar mucoid intimal edema. Immunofluorescence is negative.
Fig: Segmental thrombi with capillary wall thickening.
What is the next best step?