
Diuretic resistance is the inability to achieve euvolemia despite increasing doses of diuretic therapy. The diagnosis needs assessment of volume status and evaluation of possible contributing factors.
In general loop diuretics block a major site of sodium reabsorption, the Na-K-2Cl co- transporter (NKCC2) in the thick ascending loop of Henle and macula densa. As a result, sodium goes along the tubule taking water along with resulting in diuresis as well as natriuresis. When diuretic response is lost in heart failure two things may happen: (a) there might be insufficient delivery of loop diuretics to the proximal tubule, and (2) increased sodium hunger leading to sodium reabsorption at other nephron segments.
It can be challenging to diagnose diuretic resistance. A spot urine sodium collected two hours after administering a diuretic can help predict whether or not natriuresis will be adequate and can facilitate early recognition of an impaired diuretic response. It is however
difficult to differentiate whether this is due to insufficient loop diuretic delivery or distal sodium reabsorption

There are different ways of approaching diuretic response. As a preliminary step, it might be prudent to alter the route of loop diuretic administration (IV vs oral) or increasing the dose/ frequency.

It is important to understand some of the terminologies associated with diuretic resistance in this context. The “ceiling dose” of a diuretic refers to the single dose amount that achieves diuretic efficiency; doses above this ceiling do not meaningfully increase diuresis. The usual ceiling dose is about 80 mg of Frusemide, increased doses of oral diuretics can be required in the setting of impaired kidney drug delivery, with doses as high as 5 times being required. It is generally accepted that once the ceiling dose has been identified for an individual, this dose can be given up to every 6 hours to maximize the total daily urine output. The ceiling dose can change in an individual over time.
Apart from Furosemide, Torsemide and Bumetanide are becoming increasingly popular first
line choices due to improving costs and beneficial clinical profiles. The bioavailability is 80%-100% and are more effective than oral furosemide.
For a rough bedside conversion:
40 mg furosemide PO = 1 mg bumetanide PO/IV (most potent) = 20 mg torsemide PO/IV (longest duration of action)
One way to alleviate diuretic resistance is to reduce distal Na reabsorption. Thiazide and thiazide-like diuretics block the Na-Cl symporter in the distal convoluted tubule and the NDCBE-pendrin system in the collecting ducts. As such loop diuretics can be combined with thiazides to block the proximal as well as distal Na absorption sequentially and treat diuretic resistance – a concept referred to as “sequential nephron blockade”.
A combination regimen including four medications — a loop diuretic, thiazide, acetazolamide, and spironolactone — is called “multi-nephron segment diuretic therapy”. Multi-nephron segment diuretic therapy works at different segments of the nephron and appears to be effective in treating diuretic resistance without significant electrolyte abnormalities
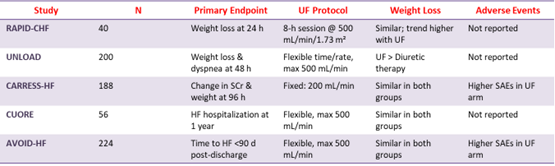
Unfortunately, there are situations in which all the diuretics in the world won’t effectively mobilize fluid. UF is the removal of isotonic fluid via convection, typically achieved using a dialysis machine. It is often considered in patients who have acute congestion refractory to multiple diuretics strategies, or those who have severe AKI or advanced CKD limiting diuretic efficacy. UF can be a short-term strategy used to support volume removal pending kidney recovery. However, there is limited data supporting its widespread use. In CARRESS-HF, UF was inferior to a stepped pharmacologic treatment strategy. UF has been associated with harm; those who were randomized to receive UF in CARRESS-HF and in the AVOID-HF
trial experienced significantly more adverse effects than those on pharmacologic treatment. The following table summarises the outcomes of UF trials in CRS 1.

Personalized medicine has the potential to significantly improve outcomes in CRS-1 by tailoring treatment based on individual patient characteristics, biomarkers, and pathophysiology.
WRF plus reduced NP = No WRF plus reduced NP ➔ Prognosis good at hospital discharge
No WRF plus no reduction NP = intermediate outcomes WRF plus no reduction/ increased NP = worse outcomes

![]()