





Clinical Case Scenario
A 70 kg 56- yr old female with acute myeloid leukaemia on induction chemotherapy with VCR- daunorubicin regimen is neutropenic day 11 following chemotherapy and admitted to ICU with confusion, facial swelling and diplopia. CECT brain reveals rhino cerebral mucormycosis and he is commenced on liposomal Amphotericin B ( LAMB) at 5mg/kg intravenous. He develops ST segment depression and T wave inversions in ECG. The following changes are noted on blood and urine parameters day 7 of therapy:



Urine output: 7500 ml/ day
Serum creatinine e: 88-242 µmol/L
Serum potassium: 4.3->3.6->2.8mmol /L
Serum magnesium :0.45 mmol /L
Serum bicarbonate 18 mol/L
Urinalysis: bland; nil casts
Renal ultrasound: normal
Which of the following statements are false regarding the mechanism of nephrotoxicity:
Clinical Scenario
A 68-year-old male with poorly controlled type 2 diabetes and peripheral vascular disease is admitted to the ICU following emergency debridement of a necrotizing soft tissue infection involving his left lower limb. He presents with septic shock: hypotension requiring norepinephrine, high-grade fever, and altered mental status. Blood cultures grow Staphylococcus aureus, and broad-spectrum antibiotics including vancomycin are initiated.
Over the next 24 hours, the patient develops oliguric acute kidney injury, classified as KDIGO Stage III, with rising creatinine and fluid overload which eventually lead to requirement of invasive mechanical ventilation. Renal replacement therapy is initiated using Coupled Plasma Filtration Adsorption (CPFA) to address both renal dysfunction and the overwhelming inflammatory response (see Figure 1).

Figure 1. Coupled Plasma Filtration Adsorption (courtesy: https://mozarcmedical.com)
Despite standard vancomycin dosing (15 mg/kg IV q12h), his trough levels remain persistently subtherapeutic at 7 µg/mL (target: 15–20 µg/mL). Repeat cultures remain positive, and clinical signs of infection persist.
Which of the following mechanisms most likely explains this finding?
Clinical Case Scenario
A 45-year-old man working as a ground cleaner for an international airline presents to the emergency department with altered mental status and oliguria. He has a history of chronic alcohol use and was found unconscious near a maintenance area with multiple empty containers of aircraft de-icing fluid. Laboratory investigations reveal a serum creatinine of 3.5 mg/dL, a high anion gap metabolic acidosis, and calcium oxalate crystals in the urine

figure 1. De-icing procedure of aircraft

Figure 2. De-icing fluid to remove ice from aircraft body
Question: What is the most appropriate initial treatment?
Clinical Case Scenario
Mr. James Thornton, a 68-year-old male with a significant medical history of uncontrolled hypertension, diabetes, and chronic kidney disease on maintenance hemodialysis, presents to the emergency department with a 3-day history of productive cough, fever, and progressive dyspnea. On initial evaluation, he is febrile, tachypneic, and hypotensive with a mean arterial pressure (MAP) of 55 mmHg and a heart rate of 110/min. He has also become oliguric for the last 8 hours and continues to be hypotensive even after receiving a fluid bolus and norepinephrine infusion. Bedside point-of-care ultrasound was performed where the Doppler profile of the LVOT demonstrated a dagger-shaped appearance (Figure 1).
What is the most appropriate next step?

Figure 1. Continuous wave doppler across LVOT (Picture courtesy-Geske JB et al.Clin Cardiol 2009;32:397)
Clinical Case Scenario
A 36-year-old female presented with history of 1 day of fever associated with rash, and breathlessness, rapidly progressing to severe metabolic acidosis, refractory septic shock requiring multiple vasopressors, acute kidney injury, and disseminated intravascular coagulopathy with multi-organ dysfunction. Physical examination revealed multiple petechial patches (Figure 2) all over the body. Despite aggressive management, including intubation, mechanical ventilation, broad-spectrum antibiotics, and fluid resuscitation, the patient’s condition deteriorates, ultimately leading to cardiac arrest and death within 36 hours of ICU admission.
A POCUS of the abdomen of this patient during resuscitation revealed the findings which are shown in figure 1. A screening echo was normal with good left ventricular systolic function. Preliminary blood culture findings show gram-negative diplococci.
Which of the following conditions best describes the rapidly progressive shock and widespread purpuric rash?

Figure 1: POCUS scan of right adrenal gland
(Case courtesy of Mohammad walid Ahmad Amin, Radiopaedia.org, rID: 192003)

Figure 2: Petechial patches on body
(Image sourced from DermNet)
Clinical Case Scenario
A 37-year-old woman with a history of type 2 diabetes mellitus arrived at the emergency department with a history of five days of worsening severe left upper quadrant abdominal pain that radiated to her left flank. She also reported fever, chills, nausea, vomiting, and general malaise. Upon arrival, her vital signs were a heart rate of 110 bpm and a axillary temperature of 39 °C. Physical examination revealed tenderness in her left costovertebral area, but her abdomen was not tender. Lab tests confirmed a urinary tract infection with a white blood cell count of 12,510 cells/mm3 and an increase in immature white blood cells. Additionally, the serum creatinine level of 5.71 mg/dL prompted the physician to perform a bedside Point-of-Care Ultrasound (POCUS) of the left kidney (figure 1) to check for urinary tract obstruction.

Figure 1: POCUS of the left kidney
(Case courtesy of Maulik S Patel, Radiopaedia.org, rID: 17283)
Which of the following POCUS findings would be most characteristic and concerning for acute emphysematous pyelonephritis?
Clinical Case Scenario
A 70-year-old man, known hypertensive managed on telmisartan and thiazide diuretic was brought to the hospital by her family due to confusion and lethargy. For the last week, he had been complaining of low oral intake. He seemed disoriented during inspection, but his hemodynamics were stable. His symptoms started around two days ago and the plasma sodium level was found to be 120 mmol/L. He experienced convulsions at the emergency room after an hour of arriving at ER and was given 3% saline to treat it. Within the following 12 hours, his blood sodium level quickly returned to 136 mmol/L. His neurological condition then worsened. An urgent MRI brain showed the following image as shown in figure 1.

Figure 1: T2 weighted imaging showing hyperintensities in basis pontis (white arrow)
(Case courtesy of Frank Gaillard, Radiopaedia.org, rID: 2598)
Which of the following best describes the pathophysiological process causing the patient’s neurological decline?
Clinical Case Secnario
A 37-year-old male with a long-standing history of chronic smoking (15 pack-years) presented to the emergency department with the acute onset of excruciating, constant, epigastric pain that radiated sharply to his back. This severe pain began approximately 12 hours before presentation and was accompanied by multiple episodes of non-bloody, bilious vomiting and complete loss of appetite (anorexia). He is a chronic smoker (15 pack years) who denies any history of alcohol abuse, recent abdominal trauma, prior surgeries, or known history of gallstones. There has been no history of recent medication intake. Upon admission, he was diagnosed with moderate acute pancreatitis secondary to severe hypertriglyceridemia (serum triglyceride 2902 mg/dL), as supported by initial lab findings and imaging (modified CT scan severity index of 6/10) (Figure 1). He also exhibited signs of systemic inflammatory response syndrome (SIRS), including a fever of 38.5°C on arrival and a respiratory rate of 30 breaths/minute.
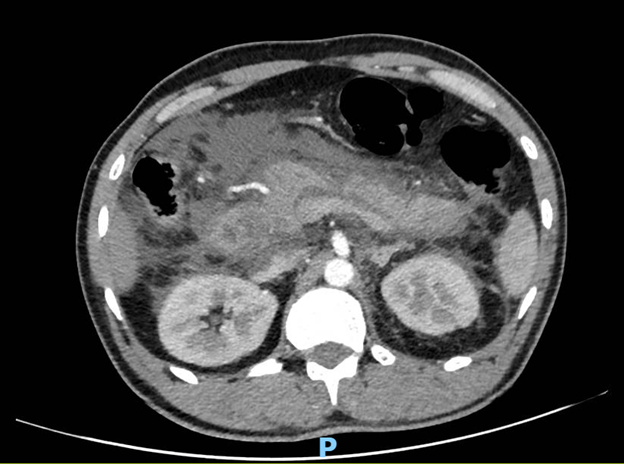
Figure 1: Contrast-enhanced CT abdomen
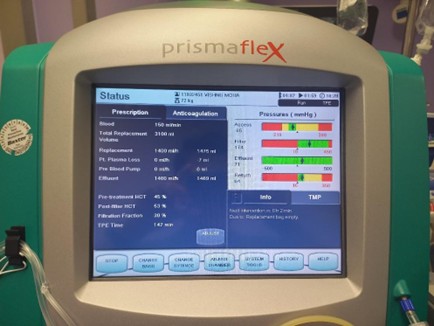
Figure 2: Settings of the extracorporeal therapy

Figure 3: Machine used for extracorporeal therapy
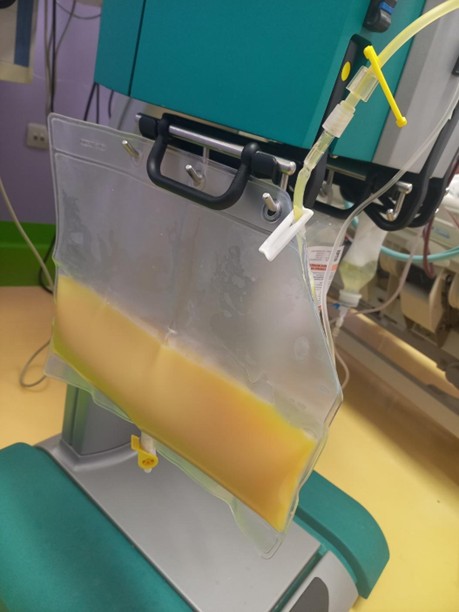
Figure 4: Filtered plasma of the patient, collected as effluent in the bag (yellowish colored as the effluent is lipemic secondary to the high level of triglycerides)
Given the patient’s presentation and the ongoing management, which of the following statements regarding the role of the extracorporeal therapy being used (Figures 2, 3, and 4) in hypertriglyceridemia-induced acute pancreatitis is most accurate?
Clinical Case Scenario
A 59-year-old man who has a history of renal transplant 3 years ago on immunosuppression suddenly developed respiratory distress, he was diagnosed with COVID-19 ARDS with a PaO2/FiO2 ratio of less than 70 for the past one day.VV-ECMO was initiated for the ARDS, he developed AKI one day post-cannulation, and his Hb was 7 g/dl. The parameters on ECMO machine and his chest X-ray are shown below:

What is the next best course of management?
Clinical Case Scenario
A 16-year-old male with a history of type 1 diabetes mellitus presented in the emergency department. His condition has worsened over the past 3 days. He reported extreme thirst and has been drinking large quantities of fluids and juice. His urine output was very high during this period, and on history taking, it was found out that he had not been compliant with his insulin regimen for the last month. His urine flow rate is measured at 12 mL/min in the emergency room using a uroflowmeter.



Despite excreting large quantities of glucose in the urine, her plasma glucose concentration remains unchanged over the observation period.
What is the primary mechanism responsible for this patient’s polyuria?
Clinical Case Scenario
A 68-year-old male with a long-standing history of chronic kidney disease secondary to poorly controlled hypertension and type 2 diabetes mellitus has been managed conservatively with dietary restrictions and medications for the past five years. His estimated glomerular filtration rate (eGFR) has been progressively declining. Over the last six months, he has developed worsening symptoms of uremia, including fatigue, nausea, loss of appetite, and pruritus. His most recent laboratory results, obtained two days ago, showed a blood urea nitrogen (BUN) of 110 mg/dL and a creatinine level of 8.5 mg/dL. He has not yet received renal replacement therapy. Today, he presents to the emergency department complaining of new-onset, sharp, retrosternal chest pain that is exacerbated by lying flat and relieved somewhat by sitting forward. He also reports increasing shortness of breath and light-headedness. His wife mentions that he seems more tired and less responsive than usual.
On physical examination, he appears pale and diaphoretic. His vital signs are as follows:
Blood Pressure: 90/60 mmHg
Heart Rate: 115 beats per minute
Respiratory Rate: 28 breaths per minute, laboured
Oxygen Saturation: 90% on room air
Auscultation of his chest reveals distant heart sounds and a soft pericardial friction rub. His jugular veins are markedly distended even when sitting upright. Peripheral pulses are weak and thready. There is no evidence of peripheral oedema on this examination.
Repeat laboratory tests show worsening azotemia with a BUN of 125 mg/dL and creatinine of 9.1 mg/dL, along with elevated potassium and phosphate levels.
The following is the echocardiography image of the patient done as a routine NephroPOCUS scan

Which of the following accurately describes a method for quantitatively evaluating this patient’s cardiac condition using echocardiography?
Clinical Case Scenario
A 35-year-old male is brought to the emergency department after being found unconscious in his apartment. His roommate reports that the patient had been complaining of severe muscle pain and dark urine for the past two days, as shown below. His roommate also described the patient having run a marathon the day prior to becoming unconscious. Upon examination, the patient’s legs are swollen and tender. Laboratory results reveal a markedly elevated creatinine kinase (CK) level of 15,000 U/L, elevated creatinine, and myoglobinuria. Although the first line of treatment for this condition is hydration with IV fluids, which of the following statements is true?

Clinical Case Scenanio
Jonathan Hayes, a 50-year-old kidney transplant recipient, presented with a gradual decline in graft function one-year post-transplant. His creatinine had risen from 1.72 mg/dL to 3.75 mg/dl with proteinuria, with a urea level of 90 mg/dL, despite unremarkable renal ultrasound findings. He remained on tacrolimus and mycophenolate mofetil, with a tacrolimus trough level of 6.4 ng/mL. Laboratory tests showed an elevated C-Reactive Protein of 28.7 mg/dL, but no obvious source of infection was identified on imaging or urinalysis, and CMV-PCR was negative. The abdominal CT-angiogram showed the following:

What can be the cause of his worsening graft function?
Clinical Case Scenario
A 57-year-old male was admitted with acute hypoxemic respiratory failure due to Influenza A pneumonia with ARDS. After an initial trial of prone ventilation failed, he was placed on veno-venous (V-V) ECMO. Initially, at low ECMO flows of 2 L/min, his pulse oximeter/peripheral oxygen saturation improved. However, as the flow was gradually increased to 4 L/min, his oxygen saturation levels worsened. A review of his chest X-ray (Figure 1) was conducted.

Figure 1: Chest Xray of the patient after cannulation
*Figure adapted from www.intensiveblog.com
Which of the following statements is true regarding the patient’s current condition?

 Where, pCO2: partial pressure of carbon dioxide, Na+ : Sodium, K+ : Potassium, Ca++ : Calcium, Mg++ : Magnesium, Cl- : Chloride Gamblegrams, named after physician James L. Gamble, are bar diagrams displaying the relative abundance of extracellular anions and cations and are commonly used to analyze acid-base disorders. Based on the gamblegrams shown below, select the appropriate combination of labels.
Where, pCO2: partial pressure of carbon dioxide, Na+ : Sodium, K+ : Potassium, Ca++ : Calcium, Mg++ : Magnesium, Cl- : Chloride Gamblegrams, named after physician James L. Gamble, are bar diagrams displaying the relative abundance of extracellular anions and cations and are commonly used to analyze acid-base disorders. Based on the gamblegrams shown below, select the appropriate combination of labels.

Clinical Case Scenario
A 38-year-old female, gravida 7, para 3, living 3, abortus 3 (G7P3L3A3) at 28 weeks of gestation with a monochorionic, diamniotic twin pregnancy underwent emergency lower segment caesarean section (LSCS) for pre-eclampsia. She was also a known case of gestational diabetes mellitus (GDM). Although her intra-operative course was uneventful, on POD 4, she developed gradually progressive and persistent abdominal pain, distension, with tenderness on palpation. A new-onset fever was noted with urine output of 250 ml over the past 24 hours. Her lab investigations on POD 4 revealed elevated C-reactive protein (CRP, 180 mg/L), and urine analysis showed leukocytes 50-100 per high-power field and positive leukocyte esterase, suggestive of UTI. Renal function tests revealed a serum creatinine of 3.4 mg/dL and BUN of 133 mg/dL. Contrast-Enhanced CT (CECT) abdomen and pelvis revealed significant free fluid in the peritoneal cavity with evidence of intraperitoneal extravasation of contrast at the dome of the bladder (Figure 1). A pigtail catheter was inserted for ascitic fluid drainage. The normal bladder anatomy is shown in the figure below (Figure 2).

Figure 1: Intraperitoneal extravasation of contrast and a clear defect in the dome of the bladder (black arrow) (Image courtesy: www.radiopaedia.org)

Figure 2: Normal bladder anatomy
Which of the following statements is incorrect regarding this case?
Clinical Case Scenario
A 22-year-old male with Burkitt lymphoma arrives at oncology day care with acute abdominal pain, nausea, vomiting, and confusion shortly after starting R-CODOX-M (rituximab, cyclophosphamide, vincristine, doxorubicin, and methotrexate). His vitals are BP 90/67 mmHg, HR 121/min, SpO2 95% on room air, and respiratory rate 25/min. Venous blood gas analysis shows: pH 7.23, PCO2 26 mmoL/L, HCO3 17 mmoL/L, Lactate 2.24 mmoL/L.
Laboratory tests reveal the following:

Despite initial aggressive intravenous fluid resuscitation and treatment with rasburicase, the patient’s urine output has dropped significantly, and he is now anuric.
Which of the following is the most likely complication this patient is experiencing?

Question 1
Which of the following statements is incorrect regarding the physiological process depicted in the figure?

Question 1

Shortly after a new Medical Renal Unit (MRU) opened, this outbreak led to 40 cases soon including deaths among patients and staff. The outbreak prompted the establishment of an advisory group led by Lord Rosenheim, which gave a series of recommendations and crucial containment measures. Despite precautions, the outbreak’s severity, had a lasting impact on infection control practices in medical settings. This outbreak in the 19th century was the subject of Colin Douglas’s popular outrageous novel “The Houseman’s Tale”, and it continues to influence the way physicians think about the risks of infection.
Choose the combination of place, year, causative organism and primary mode of outbreak transmission that is being referred to here.